





Facial rejuvenation with fillers – a two-level technique
We present the technique of applying fillers based on surgical anatomy. It is highly effective, requires little material consumption, and the results last for a long time*.
Facial aging is characterized by a number of specific phenomena occurring at approximately the same time. These are various kinds of atrophic skin changes and wrinkle formation under the influence of genetic, photochemical and environmental factors; reduction in the volume of bone and fatty facial tissue, and skin ptosis. These defects can be corrected both surgically and non-surgically, and it is characteristic that non-surgical methods are increasingly ahead of surgery in popularity.
Etiologically, volume loss mainly affects the bony skeleton and fat packs, and in a predictable pattern [2, 3]. Most often fillers are used for non-surgical volume correction. Previously, they were injected superficially with short-lived results. Today fillers are used not so much for wrinkles correction as for volume restoration. Injections are not made in the thickness of the skin, and in deep layers of soft tissue.
The technique is based on surgical concepts, the prerequisite is the long-term preservation of the result. This has been possible since the end of the last century [5] when hyaluronic acid-based gels appeared on the market, and they began to be used for volume enhancement by analogy with fat tissue transplantation. Volume restoration to a certain extent allows to reduce skin prolapse/ptosis, and also has a lifting effect.
We have been using fillers for volume augmentation for 10 years now, having changed our injection technique based on our knowledge of anatomy and a basic understanding of filler rheology.
Surgical anatomy of the aging process from a filleting perspective
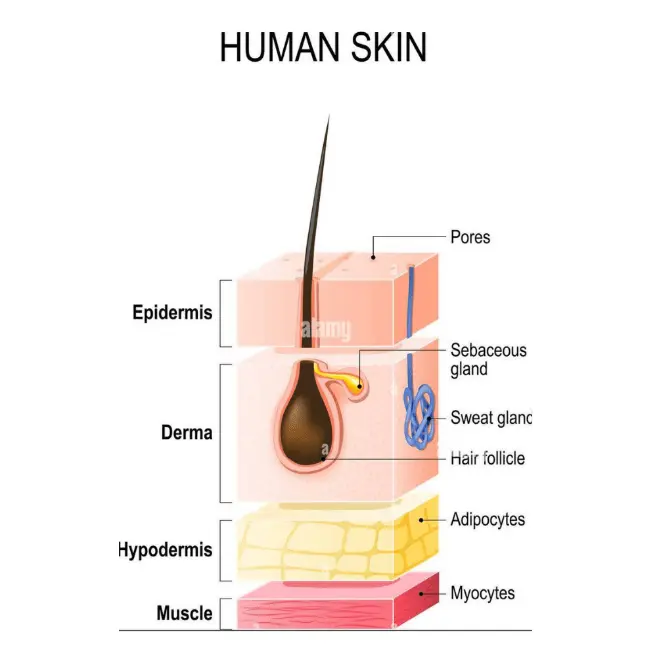
FIG. 1 Layer structure of facial tissues (“bulb”).
Facial tissues consist of several layers, similar to a bulb (Fig. 1).
With age, the bone layer undergoes resorption, mainly in the eye sockets and periorbital area, cheekbones and submandibular region, as well as in the lower jaw area.
Fat packs are depleted in a fairly predictable manner. At the deep supraperiosteal level, volume loss occurs predominantly in the area of the lateral and medial suborbital fat packs, the deep medial cheek pack and the chin pack. At the superficial subcutaneous level, this process involves the lateral packs (both in the temporal and parotid areas) and, to a lesser extent, the medial and medial fat packs of the superficial cheek fat layer. It is noteworthy that both the superficial nasolabial and upper and lower jaw packs lose less volume: they shift in the medial direction due to insufficient support from the lateral side caused by the lack of volume in the lateral fat layers and the lack of fibrous tissue fixation points (Fig. 2).
All areas of fat compartment atrophy are enclosed between the ligaments, due to which several furrows appear on the skin surface during volume reduction. These are the lacrimal sulcus and the eyelacrimal sulcus (corresponding to the ligament of the eyelacrimal sulcus and orbital supportive ligaments), the mid-cheek sulcus (malar space ligament), the nasolabial fold (nasolabial ligament), the buccal fat sulcus (temporomandibular ligament), and the puppet wrinkles (lipo-mandibular ligament) (Fig. 3). All of these ligaments tend to retain strength closer to the center of the face, where fixation remains strong, and weaken in the lateral direction.
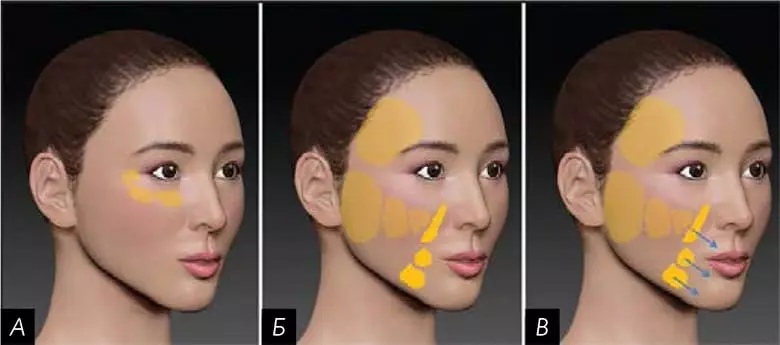
FIG. 2 A – deep fat packs of the middle third of the face, suborbital area (SOOF); B – superficial fat packs of the middle part of the face; B – displacement of the central, not subject to volume loss, superficial fat packs.
Anatomical strategy of filler injection. Two-level technique
Since the aging process of bone and fat tissue is fairly predictable, facial volume restoration procedures should be performed according to a standard protocol of sequential work on different areas of progressive atrophy in order to achieve volumetric rejuvenation of the entire face in a few sessions.
It is important to accurately select areas for injections according to the anatomy. When using the technique of two levels, first perform deep injections at the periosteum, then – surface injections into the subcutaneous fat layer. The entire treatment usually requires 3 to 5 treatments performed at 1 month intervals.
Soft tissue fillers have certain rheological properties, the most important for injectable cosmetology being viscoelasticity and cohesiveness of the material.
Viscoelasticity is a measure of the stiffnessor softness of the gel, is determined by its elasticity (modulus of elasticity, G’), i.e. how much the filler is able to restore its shape after a force, and its viscosity (viscosity modulus, G”), i.e. how the filler resists gradual deformation under the action of shear stress. Together, their values define the complex viscoelasticity modulus (G*). The higher the G* value is, the higher is the resistance to deformation and the ability to keep the shape, and thus, the expressiveness of the lifting effect.
Cohesiveness means the ability of gel particles to be held together by an external force. Gels with high cohesiveness tend to penetrate evenly into tissues and do not disintegrate into fragments during active mimicry.

FIG. 3 Projection of the main retaining ligaments of the middle and lower third of the face.

FIG. 4 Layout.

FIG. 5 “Pillars” at the deep level: several boluses per fat pack.
Processing at a deep level
Cheek area
Hyaluronic acid gels with high G* viscoelasticity are injected at the deep level in the zygomatic region, as they can have a significant lifting effect and provide volume restoration or accentuation of the desired areas without overspraying the product. Injections are performed in the lateral and medial suborbital fat packs (SOOF) and the deep medial cheek fat pack, in that order. The respective area is marked (Fig. 4), and then each fat pack is injected with a 29G or 27G needle 25 mm in length**.
To reach the bone and inject a small bolus into each pouch, a long enough needle is needed. On average, 0.3 to 0.4 ml of gel is injected into each pouch, divided into 2 to 3 separate boluses. The bolus should have a volume of no more than 0.1 – 0.2 ml to avoid compression of the lymph vessels. Thus, vertical columns are formed over the bone, supporting and raising the cheekbone area (Fig. 5). By moving from the lateral to the medial part, an overlapping effect is achieved, due to which a smaller volume of material is required in the medial parts. Augmentation of the deep medial cheek bundle provides forward tissue protrusion that is not achieved by lateral remodeling as well as reduces the nasolabial fold and recreates a youthful appearance of the cheek in its natural contours (Fig. 6).
**Pins of this length are rarely available in sets, the most common set is 13 mm. – Editor’s note
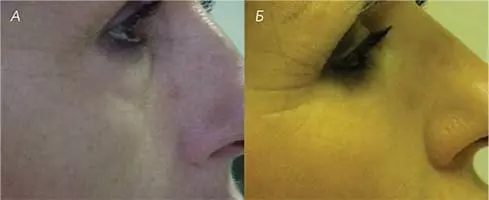
FIG. 6 Filling of the cheekbone area. A – before, B – after.

FIG. 7 Filling of the periorbital area. A – before, B – after.
Periorbital area
At the deep level in the periorbital region, high viscoelasticity G* gels are also injected as deeply as possible, directly into the periosteum. In this case, a 25G microcannula 40 – 50 mm long should be used – to avoid hematomas and to partially separate the ligamentous areas of the supporting ligaments in the periorbital region. Two access points can be selected. The first is located lateral to the external angle of the eye, in the area of the lateral ocular thickening; the cannula moves posteromedially in the direction of the secococular sulcus; the second is below the zygomatic-cosseous ligament, and the cannula is directed superior medially, cranial to the secococular sulcus ligament in the direction of the lacrimal sulcus. The average amount of material injected is 0.3-0.4 ml into the secococular sulcus and 0.1-0.2 ml into the lacrimal sulcus. In both cases, the gel is injected in small portions intermittently to avoid the formation of a “sausage” of excess filler (Fig. 7).
Lower jaw area
In the mandibular region, injections are also performed at a deep level. The drug is injected up to the periosteum with a series of vertical boluses using a 29G or 27G needle along the lower border of the mandibular bone. The area of the muzzle should be marked in advance and no injections should be made there or between the masticatory ligament, where the blood vessels pass, and the mandibular ligament. Injections in the chin are made at a deep level, directly to the bone, with the same formation of vertical columns. Even in these areas, a dense gel with a high G* viscoelasticity value should be used to achieve maximum vertical tissue elevation with minimal or no extension in the lateral direction.
Treatment of the surface subcutaneous level
After all the deep injections are done, you can move on to treating the superficial subcutaneous level. This is often done at the second appointment, usually 25 to 45 days after the first. Treatment of the superficial fat layer affects only those fat pouches that permanently lose volume, resulting in medial displacement of the other pouches.
Temporal area
In the temporal region, injections are performed superficially, in the subcutaneous tissue above the temporoparietal fascia, using a 25G microcannula 40-50 mm long. A puncture for cannula insertion is made in front of the hair growth line, carefully palpating the corresponding area to avoid hitting the superficial temporal artery. After that, the cannula is carefully introduced below, placing it parallel to the skin, slowly moving it back and forth in fan-like movements to inject the gel into the subcutaneous layer of the selected area, caudal to the temporal ridge and cranial to the zygomatic arch.
Using a cannula in this area and introducing it superficially avoids damage to numerous blood vessels as well as to the temporal branch of the facial nerve below the fascia. Cohesive gels with a small viscoelasticity index of G* should be used here so that the material can be well distributed in the fat pack and so that the effect of the filler can be improved by a modeling massage. The procedure can be completed when this area is no longer hollow, which usually happens with age, and the contour of the area between the temporal ridge and the zygomatic arch becomes flat or even slightly protruding (Fig. 8).

FIG. 8 Filling of the temporal area. A – before, B – after.

FIG. 9 Cheek lift after filing of the lateral and medial superficial fat packs. A – before, B – after.
Superficial cheek fat packet
The lateral part of the superficial cheek fat pack is treated in a similar superficial manner. Very often in the parotid region, the superficial part of the fat pack loses the most volume, so this is where you need to be especially careful to recreate the oval shape of the face. In this area, a 25G cannula 40 or 50 mm long is used, and the insertion point is located in front of the earlobe, just below the zygomatic arch. Through this point, the filler is injected into the subcutaneous layer parallel to the skin surface, performing fan-like movements, reaching the mandibular angle from below and the parotid ligament in front, which separates the lateral and middle parts of the superficial cheek fat pack.
Sometimes a second entry point is required – in front of the earlobe to completely “fill” this rather extensive anatomical area. Here, it is desirable to achieve both a volume increase and a smoothing effect, so a cohesive gel with a high G* viscoelasticity index should be chosen as the material (Fig. 9).
The middle part of the superficial cheek fat pack is medial to the parotid ligament, and this is where the next injection is made. The injection is also performed at the superficial level, in the subcutaneous layer. A 40 mm long microcannula of caliber 25G is injected into the upper lateral part of this area through the puncture. After it is inserted, it is turned in a lower-medial direction and the same fan-like movements are performed to distribute the filler evenly under the skin. Injection into this area is not always necessary, as the parotid filing often shifts it backward, creating an upward and backward vector of tension. Cohesive gels with low G’ elasticity and G’ viscosity values should be used here, spreading evenly over the subcutaneous tissue and not weighing down the area.
Injection is not always performed in the medial part of the superficial cheek fat pack, since the lifting effect after injection in the lateral and middle part is often sufficient. If you do decide to have the injection, the optimal point of entry is laterally to the corner of the mouth, next to the nasolabial fat pack. To fill this small area, a 25G cannula 40 mm long is inserted vertically upwards. A cohesive soft gel with medium G’ elasticity and G’ viscosity is suitable here, and in small quantities.
Nasolabial fold
When working with the nasolabial fold, the injection is usually made in its cranial part, where the so-called deep Ristow space is located [12]. Here gels with a high G* viscoelasticity index can be injected as deeply as possible to minimize the risk of damaging the facial artery. The caudal part of this crease is usually mobile and is only treated in patients in whom it is particularly deep. Here, the injection is made into the superficial subcutaneous tissue with a conventional 30G needle or a 25G microcannula.
In the superficial chin bundle, the injection is made with a 25G microcannula 40 mm in the direction from the mandibular ligament to the midline. A slight volume increase is also required here – just to tighten this area and reduce the nasolabial fold.
Below are the results of the above two-level technique for treating the entire face with volumetric fillers in 147 patients (146 Caucasians and 1 of Chinese origin) over the past 5 years (Table 1).
| PATIENT VOLUME | AVERAGE AGE, YEARS | NUMBER OF SESSIONS | AVERAGE AMOUNT OF DRUG PER SESSION, ML | TOTAL DRUG USED, ML |
| 147 | 47 (31—69) | 4,25 (3—8) | 3,75 | 12 |
TABLE. 1. Characteristics of the study.
Results
There were at least three sessions per patient, an average of 4.25 sessions per patient, a maximum of 8 sessions (one patient). The interval between appointments was 4 weeks (minimum 3, maximum 8 weeks). A total of 625 treatment appointments were performed. Hyaluronic acid was used as the standard filler. Six patients received polycaprolactone gel instead. An average of 12 ml per patient and 3.75 ml per procedure were used. The average amount of preparation per anatomical area on each side is shown in (Table 2).
TABLE. 1. Average amount of preparation per anatomical area on each side.
| ANATOMICAL ZONE | TOTAL, ML |
| Deep medial cheek fat | 1,5 |
| Lateral suborbital fat | 1 |
| Medial suborbital fat | 0,5 |
| Vesico-sclavicular sulcus | 0,5 |
| Lacrimal sulcus | 0,25 |
| Deep layers in the lower jaw and chin area | 2 |
| Temple | 1,5 |
| Lateral zygomatic fat pack | 2 |
| Middle zygomatic fat packet | 0,5 |
| Medial zygomatic fat packet | 0,25 |
| Chin | 1,5 |
| Nasolabial fold | 0,5 |
The most common side effects were swelling and bruising. Swelling is an expected reaction to filler injections, especially hyaluronic acid gel, which has hydrophilic properties. All patients were instructed to drink plenty of water for 3 to 4 days after the procedure and sleep on their backs with their heads elevated to reduce swelling around the injected material. In the past 3 years, all who received injections in the zygomatic and periorbital areas were prescribed betamethasone 1 mg for 2 to 3 days to avoid swelling around the eye area.
Ecchymosis after injections performed in accordance with the facial anatomy is rare because injections are usually made in areas with poor blood vessels. Injections are even less traumatic when microcannulas are used. Nevertheless, bruising (18.7%) was observed in 117 cases out of 625.
Most of the patients included in the study (124) came regularly (1 to 2 times a year) for follow-up appointments (Fig. 10). Most of them also received synergistic treatments (121 received botulinum therapy, 77 received retinoid-based home care products, 43 received thread lifting, and 13 received fractional CO2 laser resurfacing).

FIG. 10 Result before (A) and after the two-level filler procedure (B).
Seven (4.8%) patients had two other types of adverse reactions – inflammation and nodule formation. Six patients had non-specific inflammatory reactions at different times after the injection sessions, throughout the entire course of treatment. All side effects went away on their own or (in two cases) after a short course of systemic glucocorticoids. Four of these patients had minor reactions in the deep tissues with the formation of nodules. In one person, the nodules appeared without prior inflammation. In two cases, the nodules were eliminated with hyaluronidase; in all other cases, they eventually resolved on their own.
Discussion
Given the surge in popularity of noninvasive techniques, it is important to be sensitive to the anatomy and age of patients seeking augmentation and/or rejuvenation. The physician should be concerned about the safety of the patient and be guided by an aesthetic approach that takes into account the proportions. These days, whole face rejuvenation (surgical or non-surgical) involves volume restoration, tissue tightening and skin rejuvenation. Volume is only one aspect of treatment [4], and the physician must explain the entire strategy to the patient (Table 3). Aging is not a disease; however, correcting signs of aging will require accurate assessment and diagnosis. Before the patient signs a consent form and is photographed, he or she should be interviewed in detail.
| OBJECTIVES | METHODS | |
| NON-SURGICAL /SURGICAL | NON-SURGICAL | |
| Volume replenishment | Fat tissue transplantation, implants | Dermal filers |
| Tissue tightening | Facial / neck elevator | Thread lifting |
| Skin rejuvenation | Laser resurfacing/phenolic peeling | Fractional laser, skin care cosmetics |
TABLE. 1. Treatment strategies.
Biodegradable fillers meet almost all the needs of cosmetic patients and guarantee short- and long-term safety; however, several sessions are often required to achieve results because the treatment strategy involves moving from deeper levels to the surface. It also avoids overexposure, reduces the likelihood of severe swelling and bruising, and reduces the cost of each session.
From the rheological point of view, gels with a high viscoelasticity index G* have a more pronounced lifting effect [10] and are well suited for bolus injection on the supraperiosteal layer, where they form “columns” that elevate and support tissues. Gels with a small viscoelasticity index G* are better suited for work in the subcutaneous fatty tissue, where they serve as a kind of “bridges” between the columns due to their ability to expand. Often injections at a deep level are sufficient to obtain good results in terms of natural volume and tissue appearance. Superficial injections, on the other hand, allow skin tightening rather than volume increase, especially in the lateral/maxillary area.

FIG. 11 Filling of the periorbital area, before treatment (A) and at the control appointment 5 years later (B).
Most of the volume is achieved through injections at a deep level, particularly at the periosteum level, where traumatization and placement of the gel directly near the periosteum can stimulate its stem cells [14] to form new tissue, due to which the filling effect is almost permanent (Fig. 11). It is faster and more convenient to reach the bone layer using a needle: it allows the doctor to act with high precision and perfectly control the introduction of the gel. If the patient’s anatomy is studied in detail beforehand and the insertion area is carefully marked, the substance injected with the needle only reaches the bone layer under the deep fat pouches, passing by the partitions containing blood vessels. In this way, bleeding is avoided. In the deep tissues of the periorbital area, where there is a high risk of vascular perforation, it is safer to use a microcannula, especially in the area of the inner corner of the eye where the angular artery and vein pass very close to the surface.
In addition, the advantage of deep tissue injections is that most of the volume of the filler is located under the muscle. This avoids the grotesque visual effect of moving too much tissue during facial movements, as is the case if most of the product is placed intradermally or in the subcutaneous layer.
The superficial subcutaneous layer is important mainly for the lateral fat pouches, where the contours and overall shape of the face depend on it. The fusion of the temporal and parotid areas gives the effect of a beautiful contour in the area from the temporal line to the angle of the mandible, through the temporal region, the cheekbone and the back of the cheek. Accentuating the profile from the side enhances the overall result of the treatment and diminishes the “rat-face” effect seen in patients who have only the central parts of the face and lips treated. In the area of the temples and ears, only a “stretching” effect is often required, and this is provided by cohesive gels with a small viscoelasticity index of G*. The temporal area does not require a significant increase in volume, besides, it should be evenly distributed over the plane [15, 16]. The injection can be completed when the area between the temporal ridge and the zygomatic arch becomes slightly convex. In the parotid zone, slightly more volume is usually needed, so you need to distribute the gel in the plane to a lesser extent. For optimal placement of the material, it is sometimes necessary to make two insertion points: one near the ossicular ridge and one caudally in front of the earlobe.
The technique of the two levels is based on the anatomy of the deep and superficial fat packs. Accordingly, the filler must be injected into each of them separately: the material does not spread between the pouches because they are separated by fibrous septa. Each package requires a separate point of introduction of the material, so as not to get into the septum, regardless of whether you work with a needle or a cannula. After injections at the deep level, you do not need to massage the treated area – in order for the injected gel to continue to create volume. On the subcutaneous level, on the contrary, a moderate massage helps to distribute the gel so that it spreads better to the width. By filling the anatomical compartments, there is an indirect effect on the main facial furrows, because the folds arise precisely in the transition areas between the fat packs. If the filler is injected along the superficial borders between the pouches, it increases the risk of vascular damage. For example, the nasolabial fold is treated only in its fixed part.
When planning the volumization of the whole face, it is important to have a comprehensive view of the situation: to understand not only the three-dimensional structure of the areas with lost volume and explain it to the patient, but also to know before the procedures what the final result will be. Due to three-dimensional contouring by means of soft tissue augmentation, the face looks fresher and younger. Moderate volume augmentation eliminates wrinkles, and evens out wrinkles, which meets the patient’s expectations. In each area, work should be done with care so that the face looks natural and not “pumped up with fillers.”
The two-level technique is a multi-step treatment. First the deep volumes (cheekbone, eye, chin and jaw areas) are treated, then the superficial ones (temples, lateral, middle and medial zygomatic fat packs and gentle contouring of the entire face), and only after that finally work with wrinkles (if any remain) and skin quality. The results of the first procedure can be improved at subsequent corrective appointments. At the same time, patients who receive a full facial correction will require less material to maintain the aesthetic effect.
This injection technique guarantees a minimum of side effects. Those adverse events that we have observed are more likely related to the properties of the gel rather than the injection technique. Dense gels are usually more structured, which can lead to significant tissue reactions – inflammation and sometimes encapsulation of the gel. This enhanced reaction also explains the intense tissue stimulation, which results in the formation of a connective tissue capsule and the semi-permanent nature of the augmentation [14]. Injection of multiple small boluses into the area above the bone avoids cheekbone edema [17].
Once the desired volume is achieved, one session per year is sufficient to maintain the results, which is good for patients from a financial point of view. Combined with the additional effect of other non-invasive cosmetic procedures, this technique promotes the most natural course of aging, ensuring a flawless, non-conspicuous result. It is also clear that combined non-invasive therapy is associated with fewer risks than surgery and requires minimal recovery time. A continuous sequence of supportive procedures implies a whole new approach on the part of both physicians and patients, whether major manipulations or supportive treatment protocols.